Overview
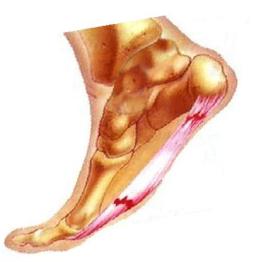
Plantar fasciitis is the most common cause of heel pain. Pain from plantar fasciitis is often most noticeable during the first few steps after getting out of bed in the morning. The plantar fascia is a thick band of tissue in the sole of the foot. Microtearing at the origin of the plantar fascia on the heel bone (calcaneus) can occur with repetitive loading. This microtearing leads to an inflammatory response (healing response) which produces the pain. Risk factors for plantar fasciitis include excessive standing, increased body weight, increasing age, a change in activity level, and a stiff calf muscle. Plantar fasciitis can be managed non-operatively in the vast majority of patients. The main components of an effective non-operative treatment program are: calf stretching with the knee straight, plantar fascia stretching, activity modification (to avoid precipitating activities), and comfort shoe wear.
Causes
Plantar fasciitis is caused by drastic or sudden increases in mileage, poor foot structure, and inappropriate running shoes, which can overload the plantar fascia, the connective tissue that runs from the heel to the base of the toes. The plantar fascia may look like a series of fat rubber bands, but it’s made of collagen, a rigid protein that’s not very stretchy. The stress of overuse, overpronation, or overused shoes can rip tiny tears in it, causing pain and inflammation, a.k.a. plantar fasciitis.
Symptoms
The heel pain characteristic of plantar fasciitis is usually felt on the bottom of the heel and is most intense with the first steps of the day. Individuals with plantar fasciitis often have difficulty with dorsiflexion of the foot, an action in which the foot is brought toward the shin. This difficulty is usually due to tightness of the calf muscle or Achilles tendon, the latter of which is connected to the back of the plantar fascia. Most cases of plantar fasciitis resolve on their own with time and respond well to conservative methods of treatment.
Diagnosis
A physical exam performed in the office along with the diagnostic studies as an x-ray. An MRI may also be required to rule out a stress fracture, or a tear of the plantar fascia. These are conditions that do not normally respond to common plantar fasciitis treatment.
Non Surgical Treatment
Management options are usually conservative. Local injection of steroids, local anaesthetic may be useful to manage symptoms. Ultrasound-guided steroid injection has been shown to be effective in short-term (four-week) pain relief and reduced thickness of the plantar fascia at three months. A posterior tibial nerve block can be performed prior for a less painful plantar fascia injection. Specific plantar fascia stretching exercises performed daily have been shown to reduce short-term (8 weeks) and long-term (two years) pain. Other supportive measures include weight reduction in obese patients, rest, non-steroidal anti-inflammatory drugs (NSAIDs) and reduction of weight-bearing pressure (soft rubber heel pad, molded orthosis, or heel cup or soft-soled shoes).

Surgical Treatment
If treatment hasn’t worked and you still have painful symptoms after a year, your GP may refer you to either an orthopaedic surgeon, a surgeon who specialises in surgery that involves bones, muscles and joints, a podiatric surgeon, a podiatrist who specialises in foot surgery. Surgery is sometimes recommended for professional athletes and other sportspeople whose heel pain is adversely affecting their career. Plantar release surgery. Plantar release surgery is the most widely used type of surgery for heel pain. The surgeon will cut the fascia to release it from your heel bone and reduce the tension in your plantar fascia. This should reduce any inflammation and relieve your painful symptoms. Surgery can be performed either as, open surgery, where the section of the plantar fascia is released by making a cut into your heel, endoscopic or minimal incision surgery – where a smaller incision is made and special instruments are inserted through the incision to gain access to the plantar fascia. Endoscopic or minimal incision surgery has a quicker recovery time, so you will be able to walk normally much sooner (almost immediately), compared with two to three weeks for open surgery. A disadvantage of endoscopic surgery is that it requires both a specially trained surgical team and specialised equipment, so you may have to wait longer for treatment than if you were to choose open surgery. Endoscopic surgery also carries a higher risk of damaging nearby nerves, which could result in symptoms such as numbness, tingling or some loss of movement in your foot. As with all surgery, plantar release carries the risk of causing complications such as infection, nerve damage and a worsening of your symptoms after surgery (although this is rare). You should discuss the advantages and disadvantages of both techniques with your surgical team. Extracorporeal shockwave therapy (EST) is a fairly new type of non-invasive treatment. Non-invasive means it does not involve making cuts into your body. EST involves using a device to deliver high-energy soundwaves into your heel. The soundwaves can sometimes cause pain, so a local anaesthetic may be used to numb your heel. It is claimed that EST works in two ways. It is thought to, have a “numbing” effect on the nerves that transmit pain signals to your brain, help stimulate and speed up the healing process. However, these claims have not yet been definitively proven. The National Institute for Health and Care Excellence (NICE) has issued guidance about the use of EST for treating plantar fasciitis. NICE states there are no concerns over the safety of EST, but there are uncertainties about how effective the procedure is for treating heel pain. Some studies have reported that EST is more effective than surgery and other non-surgical treatments, while other studies found the procedure to be no better than a placebo (sham treatment).